
Dr Akash Malik-MD
Senior Programme Officer, Global Development - Gates Foundation
Climate change is often described through images of melting glaciers, rising seas, dry rivers, and burning forests. These images are important, but they can make the issue feel distant from daily life. From a public health perspective, climate change is much closer. It affects the air people breathe, the water they drink, the food they eat, the infections they face, the safety of pregnancy, the health of children, and even mental well-being. Climate change is therefore not only an environmental concern; it is a population health emergency. The central message is simple: when the climate changes, the conditions required for health also change.
Science is now very clear. Human activity, especially the burning of coal, oil, and gas, has warmed the planet by about 1.1°C above the 1850-1900 baseline. The Intergovernmental Panel on Climate Change (IPCC) has concluded that human influence is unequivocally responsible for warming the atmosphere, ocean, and land. Each of the last four decades has been warmer than any previous decade since 1850 (IPCC, 2023). A change of 1.1°C may sound small, but this is a global average. It translates into more frequent heatwaves, heavier rainfall, longer droughts, stronger cyclones, rising sea levels, and more unstable disease ecology.
A useful way to understand this is to distinguish weather from climate. Weather is what happens today or this week: a hot afternoon, a storm, rainfall, or humidity. Climate is the long-term pattern of weather over decades. Climate variability refers to shorter natural fluctuations such as El Niño or changes in monsoon behaviour. Climate change means that the background conditions are shifting. This makes extreme events more likely, more intense, and more damaging. For public health systems, this means that yesterday's planning assumptions may no longer be reliable.
Greenhouse gases are at the centre of this change. The atmosphere is mostly nitrogen and oxygen, but trace gases such as carbon dioxide, methane, nitrous oxide, and ozone trap heat. This natural greenhouse effect keeps Earth livable. The problem is that human activity has added too much of these gases, trapping extra heat. Carbon dioxide is the reference gas, with a global warming potential of 1. Methane has about 27-30 times the warming potential of carbon dioxide over 100 years, while nitrous oxide has a global warming potential of around 273. Some industrial gases are even more powerful. This means that even small concentrations can have large climate effects.
The scale of health risk is already large. The World Health Organization estimates that 3.6 billion people live in areas highly susceptible to climate change. Between 2030 and 2050, climate change is expected to cause about 250,000 additional deaths every year from undernutrition, malaria, diarrhoeal disease, and heat stress alone. Direct health damage costs are projected at US$2-4 billion per year by 2030, not including damage to agriculture, water systems, infrastructure, or productivity. These numbers are conservative because they do not fully capture mental health, displacement, noncommunicable diseases, or health-system disruption.
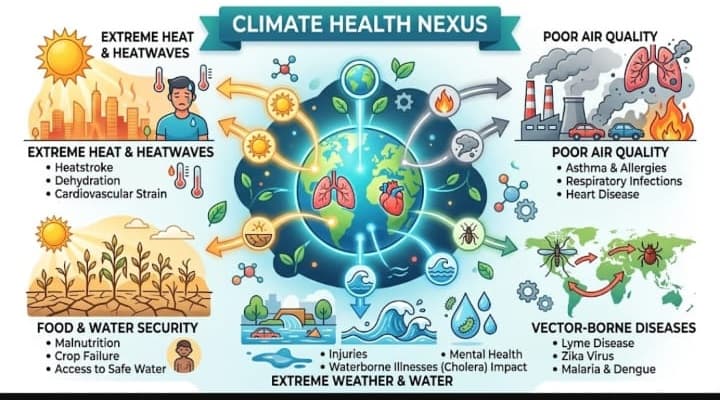
Climate harms health through both direct and indirect pathways. Direct harms include heat stroke, dehydration, injuries, drowning, burns, and smoke inhalation during extreme weather events. Indirect harms occur through changes in air quality, water quality, food security, vector ecology, livelihoods, migration, and social stability. A large overview of 94 systematic reviews found that climate change is associated with worse human health across several domains, with infectious diseases, mortality, and cardiorespiratory outcomes among the most frequently studied outcomes.
Heat is one of the clearest and deadliest hazards. Heat illness exists on a spectrum. Mild illness may begin with cramps, dizziness, or fainting. Heat exhaustion can cause weakness, nausea, heavy sweating, and dehydration. Heat stroke is life-threatening; body temperature rises above 40°C, the brain is affected, and multi-organ failure can follow. But heat does not kill only through classical heat stroke. It worsens heart disease, stroke risk, kidney disease, diabetes, respiratory illness, and mental health conditions. Older people, infants, pregnant women, outdoor workers, people with chronic disease, and those living in poorly ventilated homes are especially vulnerable.
The health effects of heat are strongly linked to social conditions. A wealthy household may use air conditioning, filtered water, and private transport. A construction worker, sanitation worker, farmer, traffic police officer, or street vendor may spend long hours in direct sun with limited access to shade, rest, toilets, or drinking water. In cities, concrete surfaces create urban heat islands, making poorer neighbourhoods hotter. This is why heat action plans must go beyond alerts. They need public drinking water, shaded work areas, cool roofs, adjusted work timings, community outreach, emergency care readiness, and protection for high-risk workers.
Climate change and air pollution are twin crises. Both are driven by fossil fuel use, and both damage health. Air pollution is estimated to cause around 7 million premature deaths each year globally, and 99% of the global population breathes air that exceeds WHO guideline limits. Fine particulate matter, ground-level ozone and other pollutants increase asthma, chronic obstructive pulmonary disease, heart attacks, stroke, lung cancer, and adverse pregnancy outcomes. The public health opportunity is large: reducing fossil fuel burning can improve air quality almost immediately while also slowing climate change-air-quality-and-health).
Respiratory health is affected through many routes. Higher temperatures increase ground-level ozone formation. Wildfire smoke exposes large populations to fine particulate matter, carbon monoxide, and toxic compounds. Longer pollen seasons worsen allergic rhinitis and asthma. Floods and damp housing increase mould exposure. Children, older adults, and people with asthma or chronic obstructive pulmonary disease are particularly affected. These impacts are not limited to disaster periods; they may become part of routine outpatient and emergency care workloads.
Vector-borne diseases are another major concern. Temperature, rainfall, and humidity affect where mosquitoes, ticks, and other vectors can survive. Warmer temperatures can shorten the extrinsic incubation period, meaning pathogens may develop faster inside mosquitoes. Altered rainfall can create new breeding sites. Urban heat islands and water storage can support Aedes mosquitoes, increasing dengue and chikungunya risk. Climate change may also shift malaria transmission to new altitudes and regions, while diseases such as Japanese encephalitis, leishmaniasis, Lyme disease, Zika, and West Nile virus may change their range and seasonality. Public health surveillance must therefore become climate-informed.
Water, sanitation, and hygiene risks also increase. Floods can contaminate drinking water sources and damage sanitation systems. Droughts reduce water quantity and concentrate pollutants. Warmer water can support the growth of pathogens such as Vibrio species. After floods, communities may face diarrhoea, cholera, typhoid, hepatitis A and E, leptospirosis, and skin infections. Food safety is also affected because heat accelerates bacterial growth, power cuts disrupt cold chains, and floodwater can contaminate fresh produce. Climate adaptation must therefore include resilient water supply, sanitation, drainage, food safety monitoring, and outbreak preparedness.
Food and nutrition are central to climate-health risk. Heat, droughts, floods, and changing rainfall reduce crop yields and threaten fisheries and livestock. Higher carbon dioxide can reduce the nutrient density of some crops, including protein, zinc, and iron content. Food prices rise when production falls, pushing poorer households toward cheaper and less nutritious diets. For children, this can mean wasting, stunting, micronutrient deficiencies, and long-term cognitive impacts. For pregnant women, it can mean anaemia, poor weight gain, and higher obstetric risk. Climate change is therefore also a nutrition and food-security challenge.
Pregnancy and newborn health deserve special attention. A recent systematic review and meta-analysis found that heat exposure is associated with adverse maternal, fetal, and neonatal outcomes. The review reported that each 1°C increase in heat exposure was associated with increased odds of preterm birth, and that heatwaves were associated with substantially higher odds of preterm birth. It also found harmful associations with stillbirth, gestational diabetes, congenital anomalies, and other obstetric complications. This matters deeply for countries with large pregnant populations, high heat exposure, and uneven access to cooling and timely care.
Children are among the most vulnerable. UNICEF's Children's Climate Risk Index found that about 1 billion children live in countries at extremely high risk from climate and environmental hazards (UNICEF, 2021). Children breathe more air per kilogram of body weight, develop immune and thermoregulatory systems, spend more time outdoors, and depend on adults for protection. Climate change increases their risk of diarrhoeal disease, malnutrition, asthma, dengue, malaria, heat stress, school disruption, and mental distress. Protecting children must be a core measure of climate policy success.
Mental health is often under-recognised, but it is a major part of climate health. Disasters can cause grief, trauma, anxiety, depression, and post-traumatic stress disorder. Repeated crop loss, debt, displacement, and livelihood insecurity create chronic stress. Young people increasingly report anxiety about the future of the planet. People may also experience distress when familiar environments, such as farms, rivers, or forests, are damaged. Mental health services, psychological first aid, social protection, and community support should be included in disaster response and climate adaptation plans.
India is highly exposed to these risks. The Council on Energy, Environment and Water found that more than 75% of Indian districts, home to over 638 million people, are hotspots for extreme climate events (Council on Energy, Environment and Water [CEEW], 2021). India faces heatwaves, floods, droughts, cyclones, glacial risks, urban flooding, air pollution, and changing vector patterns. The health burden will not be evenly distributed. Outdoor workers, farmers, women, children, older adults, migrants, coastal communities, tribal populations, urban poor households, and people with chronic illnesses will face higher exposure and lower protection.
This is why climate justice is health justice. The populations least responsible for historical emissions often face the worst health consequences. The IPCC has shown that mortality from floods, droughts, and storms was 15 times higher in highly vulnerable regions than in regions with very low vulnerability between 2010 and 2020. Within countries, the same pattern appears between rich and poor households. Effective climate action must therefore be equity-focused, not only technology-focused.
The way forward has two pillars: mitigation and adaptation. Mitigation means reducing greenhouse gas emissions through clean energy, public transport, energy efficiency, reduced fossil fuel use, sustainable agriculture, afforestation, and better waste management. Adaptation means preparing for the impacts already happening: heat action plans, early warning systems, resilient water and sanitation, climate-informed disease surveillance, emergency preparedness, cool roofs, flood-safe health facilities, and climate-resilient primary healthcare. Mitigation prevents the causes; adaptation manages the impacts. Both are essential.
Health systems must now become climate-resilient. Primary health centres and hospitals should remain functional during heatwaves, floods, power cuts, and outbreaks. Health workers should be trained to recognise heat illness, dehydration, climate-sensitive infections, mental distress, and risks during pregnancy. Surveillance should track heat morbidity, vector-borne disease, diarrhoeal outbreaks, air pollution alerts, and climate-sensitive deaths. Supply chains for medicines, vaccines, diagnostics, oxygen, and emergency supplies must be protected from extreme weather disruption. The WHO operational framework for climate-resilient and low-carbon health systems provides a practical roadmap covering governance, workforce, vulnerability assessment, early warning, infrastructure, health programmes, and financing (WHO, 2023c).
Community medicine has a unique role at this interface. Public health professionals can map vulnerable populations, conduct local vulnerability assessments, support heat action plans, strengthen disease surveillance, design risk communication, train frontline workers, coordinate with other departments, and generate local evidence. They can translate climate science into practical advice: drink water before thirst, avoid peak heat, check on older adults, remove stagnant water, use oral rehydration solution during diarrhoea, protect pregnant women from heat exposure and seek early care after floods or fever outbreaks.
The hopeful message is that climate action improves health immediately. Cleaner energy reduces air pollution. Safer walking and cycling reduce obesity, diabetes, and heart disease. Greener cities reduce heat islands and improve mental well-being. Sustainable diets can improve nutrition. Stronger primary healthcare improves preparedness for both disasters and routine illness. In this sense, climate action is not a burden added to health systems; it is a route to healthier, fairer, and more resilient societies.
The conclusion is clear. Climate change is not a distant future threat and is not only an environmental issue. It is already shaping disease patterns, deaths, pregnancy outcomes, childhood health, mental well-being, livelihoods, and health-system performance. For India and other climate-vulnerable settings, the choice is not between development and climate action. The real task is to make development climate-smart, health-centred, and equity-focused. Protecting the climate is now one of the most practical ways to protect human health.
• Council on Energy, Environment and Water. (2021). Preparing India for extreme climate events: Mapping hotspots and response mechanisms. CEEW.
• Intergovernmental Panel on Climate Change. (2023). Climate change 2023: Synthesis report. Contribution of Working Groups I, II, and III to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. IPCC. https://doi.org/10.59327/IPCC/AR6-9789291691647
• Lakhoo, D. P., et al. (2025). A systematic review and meta-analysis of heat exposure impacts on maternal, fetal, and neonatal health. Nature Medicine, 31, 119-128. https://doi.org/10.1038/s41591-024-03395-8
• Rocque, R. J., Beaudoin, C., Ndjaboue, R., Cameron, L., Poirier-Bergeron, L., Poulin-Rheault, R.-A., Fallon, C., Tricco, A. C., & Witteman, H. O. (2021). Health effects of climate change: An overview of systematic reviews. BMJ Open, 11(6), e046333. https://doi.org/10.1136/bmjopen-2020-046333
• UNICEF. (2021). The climate crisis is a child rights crisis: Introducing the Children's Climate Risk Index. United Nations Children's Fund.
• World Health Organization. (2023a). Climate change and health. https://www.who.int/news-room/fact-sheets/detail/climate-change-and-health
• World Health Organization. (2023b). Ambient (outdoor) air pollution. https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health
• World Health Organization. (2023c). Operational framework for building climate-resilient and low-carbon health systems. World Health Organization.

